




Imagine that you went to a doctor for athlete’s foot and they said, “We have fifteen different treatment options, and I’m going to present them to you in alphabetical order.” Imagine that the doctor did this despite the fact that some of the methods worked ten times better to fix your condition. Even for something as minor as foot fungus, that just seems like bad medical care. You know your body, but they know the world of medicine. It’s their job to differentiate, and after checking for possible allergies, lifestyle patterns and so forth, to recommend whatever is most likely to get the job done. Now imagine that there were five kinds of COVID vaccine, and some worked ten or even 100 times as well as others, and the doctor presented them to you in alphabetical (or random) order. You might think that was incompetence or malpractice.
But that is how some reproductive health providers treat birth control options.
Consider, for example, the generally well regarded Reproductive Health Access Project, which supports clinicians who provide contraceptive and abortion care, and miscarriage management. Among other tools in their store is a “patient fact sheet” titled Your Birth Control Choices that they promote and sell. Their website describes the fact sheet thus: “This patient fact sheet compares different birth control choices in a colorful and easy-to-read chart. . . . Ideal for health centers, doctor’s offices, and school clinics.”
But the sheet doesn’t lead with the methods that are most likely to help patients seeking birth control actually attain their top goal, meaning those that work best to prevent unwanted surprise pregnancies. It’s in alphabetical order. And it just so happens that alphabetical order puts some of the very least reliable methods at the top, where people might normally expect the best. To make matters worse, all of the most trustworthy and genuinely modern methods—various kinds of pills, IUDs and implants, are relegated to the back side and don’t even show up if someone is just scanning their website.
Take a look.

If you squint, what you’ll see is that the leading methods are condoms and diaphragms—methods that are now more than half a century old, and each of which can be expected to fail for somewhere between 10-20 percent of users each year.
A few years ago I was cleaning out my mother’s house so that she could move into a retirement community, when I came across a small blue box tucked into the headboard of her bed. I’m the oldest of six children, and when I opened the box what I found was her diaphragm—and five little maternity ward baby bracelets.
 |
| Mom’s Diaphragm with Five Baby Bracelets |
Five diaphragm babies. And sixty years later that is what the Reproductive Health Access Project is showcasing top-of-the-fold, Page One.
Three years ago, before Your Birth Control Choices was revised, it aligned more with what one might expect from a menu of medical options—it led, as people generally trust their doctors to do, with the stuff that was most likely to work. Now the opposite is true. And because we know that people are modestly more likely to choose from the top of the list when they don’t have a strong preference, this new exception to standard medical practice means that more people are going to end up with a mistimed or unwanted pregnancy.
What is going on here?
What’s going on is a misguided attempt to avoid anything suggesting that healthcare providers have opinions or preferences when it comes to what kind of treatment or prevention they deliver. It is precisely because people are somewhat more likely to choose the headline option, that long-acting IUDs and implants (the kind of contraception most often preferred by reproductive care providers for themselves and their family members, by the way) are no longer there. Some advocates in reproductive justice nonprofits conflate leading with LARC (long-acting reversible contraception), with nudging, with pressuring, with coercing, with forcing—with the unconsented sterilizations that took place during the early part of the 20th century and that disproportionately affected Black women.
Reproductive coercion is worth worrying about. Throughout human history women have been pressured, threatened, and raped into bearing children—as economic assets for their husbands or masters, as foot soldiers for the state, and as devotees to the gods. They have been sterilized or forced to use fail-safe contraceptives when someone else decided that their tribe was too degenerate or prolific. With America in the middle of a racial reckoning, this history and this threat are front and center.
The folks who decided to alphabetize birth control options are swimming in this sea. And no doubt they genuinely mean to protect reproductive freedom. But if so they should remember that even in their own movement, it’s not the thought that counts—it’s the effect. Leading with a diaphragm that will fail almost 1 in 5 women during a single year over an implant that will fail 1 in 2000 leads to less reproductive empowerment, not more. One might think of it, in fact, as a form of stochastic coercion: You don’t know who is going to get forced by contraceptive failure into a baby they didn’t want, but you know for sure that someone will.
Some social justice advocates have become so focused on fixing conversational dynamics and social standing—what words we use, who sits where in which pecking order—that they have lost interest in the practical tools that build equity and opportunity—things like education, and living wage jobs, and reliable family planning.
With the Religious Right trying to force pregnant people to act as incubators and then give birth, with GOP appointees stripping away the safest and most effective forms of abortion care, one might think that the Left would be deeply invested in letting people know about the most trustworthy contraceptives around—and in broad uptake by those who find their interest piqued.
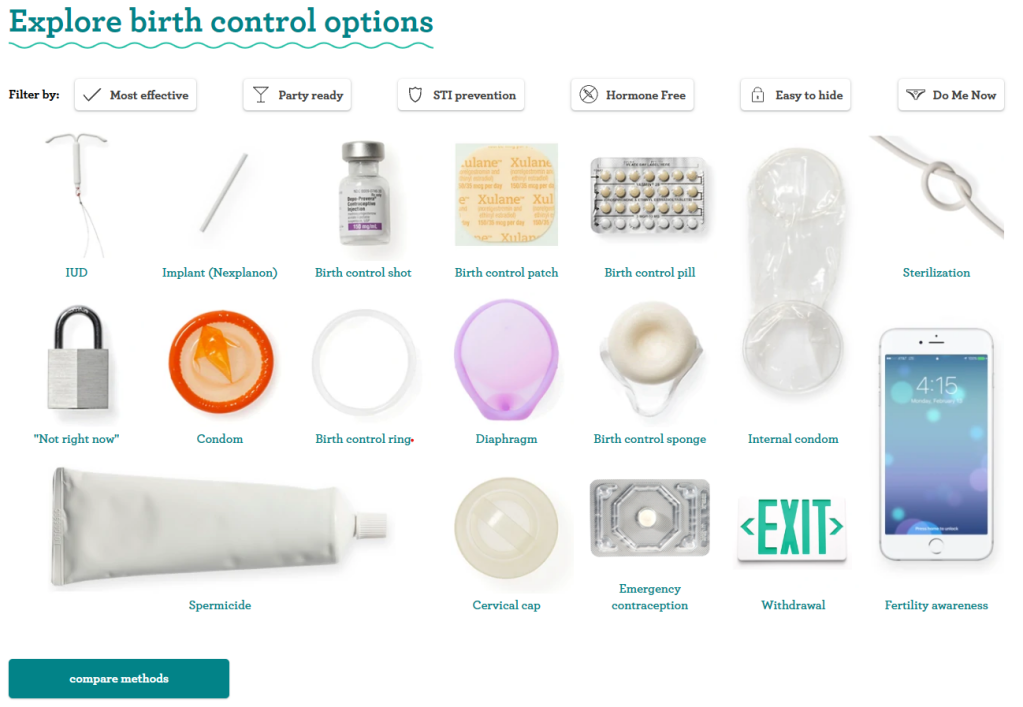
One way to reduce unmet need for abortion is to reduce need for abortion. And the most powerful means we have of doing that is to ensure that everyone knows about state-of-the-art contraceptives that take human error out of the equation for months or even years at a time until a person decides they want a child. Birth control is a personal decision, and no one method suits everyone. But trustworthy birth control is power. People deserve to know that some options drop the risk of an unwanted pregnancy to near zero–and others don’t. That information is right up front at Bedsider.org for example, which provides up-to-date information about birth control to the general public.
Bedsider.org Explore Birth Control Options
 Why is their chart organized the way it is? Here’s why.
Why is their chart organized the way it is? Here’s why.
Two years ago one of my friends was diagnosed with brain cancer. When she talked to her doctor, she wanted to know all of her options. But she sure as hell also wanted a medical opinion about which course of treatment would best stack the odds in her favor. Alphabetizing is for people who have long lists of information to sort through. It’s for finding things in a hurry when you know what you are looking for, and it works very well for that. But it is no substitute for thoughtful input from a medical professional, one who explores what you are trying to accomplish and then offers their knowledge of what might work to get you there.
Three years ago, before Your Birth Control Choices was revised, it aligned more with what one might expect from a menu of medical options—it led, as people generally trust their doctors to do, with the stuff that was most likely to work. Now the opposite is true. And because we know that people are modestly more likely to choose from the top of the list when they don’t have a strong preference, this new exception to standard medical practice means that more people are going to end up with a mistimed or unwanted pregnancy.
What is going on here?
What’s going on is a misguided attempt to avoid anything suggesting that healthcare providers have opinions or preferences when it comes to what kind of treatment or prevention they deliver. It is precisely because people are somewhat more likely to choose the headline option, that long-acting IUDs and implants (the kind of contraception most often preferred by reproductive care providers for themselves and their family members, by the way) are no longer there. Some advocates in reproductive justice nonprofits conflate leading with LARC (long-acting reversible contraception), with nudging, with pressuring, with coercing, with forcing—with the unconsented sterilizations that took place during the early part of the 20th century and that disproportionately affected Black women.
Reproductive coercion is worth worrying about. Throughout human history women have been pressured, threatened, and raped into bearing children—as economic assets for their husbands or masters, as foot soldiers for the state, and as devotees to the gods. They have been sterilized or forced to use fail-safe contraceptives when someone else decided that their tribe was too degenerate or prolific. With America in the middle of a racial reckoning, this history and this threat are front and center.
The folks who decided to alphabetize birth control options are swimming in this sea. And no doubt they genuinely mean to protect reproductive freedom. But if so they should remember that even in their own movement, it’s not the thought that counts—it’s the effect. Leading with a diaphragm that will fail almost 1 in 5 women during a single year over an implant that will fail 1 in 2000 leads to less reproductive empowerment, not more. One might think of it, in fact, as a form of stochastic coercion: You don’t know who is going to get forced by contraceptive failure into a baby they didn’t want, but you know for sure that someone will.
Some social justice advocates have become so focused on fixing conversational dynamics and social standing—what words we use, who sits where in which pecking order—that they have lost interest in the practical tools that build equity and opportunity—things like education, and living wage jobs, and reliable family planning.
With the Religious Right trying to force pregnant people to act as incubators and then give birth, with GOP appointees stripping away the safest and most effective forms of abortion care, one might think that the Left would be deeply invested in letting people know about the most trustworthy contraceptives around—and in broad uptake by those who find their interest piqued.

One way to reduce unmet need for abortion is to reduce need for abortion. And the most powerful means we have of doing that is to ensure that everyone knows about state-of-the-art contraceptives that take human error out of the equation for months or even years at a time until a person decides they want a child. Birth control is a personal decision, and no one method suits everyone. But trustworthy birth control is power. People deserve to know that some options drop the risk of an unwanted pregnancy to near zero–and others don’t. That information is right up front at Bedsider.org for example, which provides up-to-date information about birth control to the general public.
Bedsider.org Explore Birth Control Options

Two years ago one of my friends was diagnosed with brain cancer. When she talked to her doctor, she wanted to know all of her options. But she sure as hell also wanted a medical opinion about which course of treatment would best stack the odds in her favor. Alphabetizing is for people who have long lists of information to sort through. It’s for finding things in a hurry when you know what you are looking for, and it works very well for that. But it is no substitute for thoughtful input from a medical professional, one who explores what you are trying to accomplish and then offers their knowledge of what might work to get you there.
 |
Valerie Tarico is a psychologist and writer in Seattle, Washington. She writes about religion, reproductive health, and the role of women in society. |



{kind=link}
No comments